| Home What we do Storytelling for User Experience Articles and downloads About us |
|
What do we mean by user friendly? by Whitney Quesenbery I was really pleased this morning to hear Dr. Ahern talk about user-centered design. It is great that we're hearing it from the top of the profession, because out in the trenches, the glass is maybe about an eighth full. There's a wonderful: "The future is already here. It's just not evenly distributed.” That’s certainly true in healthcare. One of our challenges is to get from some of the really fabulous ideas about what we can do with technology and how we can improve health care into the actual screens or devices in front of actual people -- both patients and health care professionals. Only then will what we know about usability be able to make a difference in healthcare. Is the public ready for eHealth information?
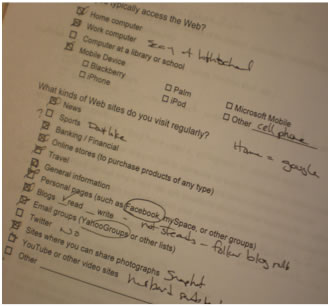
In the beginning, we hardly saw anyone who claimed to use – or even know about – popular social media tools. More recently, we are seeing the same shift that we see in the quantitative demographic data: the web has gone from something that's unusual or that used only at work to something everyday and normal. Instead of asking how many hours a day or week people use the way, we ask if it is “part of your daily life, something you use only at work, or something you use just when you need it.” They look at us in bewilderment and they say "It's part of my daily life. It's how I get directions, it's how I do everything." So, the question is not whether the public is ready for e-health information but whether we're ready to meet their expectations. Because while we've been building big systems, the world has been moving on. We have a lot of expectations for self-supportWe have expectations for self-service. With support. Any time. Connecting people. On any device.
People expect support, including both online support and a real person behind that support when they have a more complicated question. The lines between online and offline are much blurrier than they used to be. They want to do it any time any place. Ask somebody how convenient they want it, they say "I want it very convenient." We recently asked people what hours they think the NCI’s Cancer Information Service should be available for phone, email and online chat. They turned to me and says “Well, all 24 hours. I know that’s probably not practical, but it should be 24 hours.” They know what the realities are, but we have to face the fact that they want information any time they need it. They want to connect with people, whether that’s an online circle of friends, in the anonymity of a forum, or in person. And they are trying out different ways to do this. Families using Twitter to let everyone know that Dad is awake and now is a good time to call him. Or sites like PatientsLikeMe that trade your own medical information for access to the tactics and strategies of others like you. They want to do it on the device they choose. We are seeing people who have 2 and 3 phone, a netbook, their home computer and their work computer. When we ask which devices they use to get healthcare information, they say, "It depends on where I am and which is more convenient to use at that moment." We need to see people as individuals…not just “demographics”In usability and user experience design, we use a tool called “personas” to help us picture the people we are designing for. Personas wrap up demographic data, qualitative data, and details like attitudes and their preferred formats for information into a portrait of a person. At cancer.gov, this might mean thinking about their needs at different places along the cancer journey. One of advantage of working in a place like National Cancer institute – and probably anywhere in healthcare – is that not only do we have a lot of high-quality quantitative data, but also strong connections to the human context. One of the challenges of most technology projects is that the users are rarely in the room when they are created. We have health information specialists, designers and other health professionals, but there is rarely a patient actively working on a project. One of the values of these personas is that they help us keep the people who we are actually working for present for us. This is not just a challenge in healthcare, but in how too many information technology projects are organized: developers work in “cubie farms” – environments that make it difficult to have any real connection to the context in which their work will be used. This allows the systems analysis to be so abstract that it can ignore the way people actually work. As an example, I worked on a hospital information system. In the models for messaging within the hospital, no one thought about the fact that the clinic receptionist and scheduling clerk might be sitting within three feet of each other. Surely the real environment must make a difference to the way we design applications to support those roles!
Both might want to be sure that it is error tolerant, that it helps them not only prevent errors, but to undo mistakes. Information and technology the way they want it.A few years ago at the Usability Professionals’ Association conference a doctor gave a talk about computers and medicine. Someone in the audience asked, "Why won't physicians use computers?" His answer was something like, “We use computers all the time. We just won't use your stinking computers” His problem was that most of the systems at the time were designed to manipulate data, not fit into a clinical environment and help clinicians with their tasks. Our challenge is to design systems that are not only powerful enough to handle the volume of information and the complexity of the data, but which also support both patients and professionals, helping them do their work. It's very easy for us to think about things we want to push to people, things we want people to do. As an example, every social media site I've signed up for lately wants to send me messages. One which I signed up to get a nice itinerary for my travel, wants to connect me to friends who might be in that city. Maybe I want that and maybe I don't. Maybe I want messages every day asking me if I’ve exercised and maybe I don't? But what happens when I'm on five of these programs and all of them are sending me messages. Or 10 systems, or 15 systems? As designers, we think about our narrow slice of life and what our system is going to do and forget about the overall ecology and the environment in which that comes in. Do I want to be in a meeting and have a health alert pop up on my work e-mail? How do we begin to help people separate their private lives from their public lives ? Usability and accessibility are defined in terms of peopleUsability is a quality of product, but it is defined in the terms of people.
And there's an ISO standard (ISO 9241-20:2008) that simply defines accessibility as usability for a broader group of people – people with the widest range of capabilities. This definition allows us to get away from the notion that accessibility is about screen readers. Instead we can focus on the person behind the screen reader and making sure they can have the same or equivalent experience as everyone else. I work for The Open University which takes accessibility very seriously. During one of our regular usability tests, we included remote sessions with people who use assistive technology. When we looked at the data, we were surprised (and happy) to see that their comments the usability of the site were the same as the comments we heard from other people. It was impossible to tell which participants had a disability and which did not. This, to me, is a great achievement. It means that we're past fundamental barriers and moving on to actually making things that work for people. It’s time to start aiming for broad, broad inclusion and to make sure we're not leaving people out because they're inconvenient to work for. We also need to think about how and when we set standards. This is always a delicate point. If standards are set too early, they can stifle innovation. But if we standardize too late, the standards get set at a very low common denominator. They may set a few technical points, but they don’t address the real usability and accessibility needs of the real people who have to use them, because they are not written around broad goals for usability and accessibility. Usabilty and accessibility have to be designed in.The real tragedy is that an industry can go from “it’s too early to standardize” to being too late for meaningful standards in what seems like a blink of the eye. We end up with a proliferation of incompatible systems, which all work differently. If we don't start thinking about inclusion from the very beginning of a project, start thinking about not just telemedicine but how we're going to make sure that people who are blind or using screen readers can access it. If we don’t think about different ways people might access it – from a tablet computer or a mobile device; with keyboard or voice. And where and when they might need access. If we don’t consider the broad range of people, there is no way the products we design will meet the goals for usability and accessibility for that broadest range of people with that widest range of capabilities. There's a wonderful quote from Clayton Lewis that says usability can't be “smeared on top like peanut butter." They are not decoration. If usability and accessibility are not structurally part of the product, then it's too late to do it right and we have to simply wait for the next generation when we can tear it down and start again.
Thank you.
This talk was part of a panel on usability and accessibility, moderated by Bettijoyce B. Lide, National Institute of Standards & Technology at Informatics for Consumer Health: Summit on Communication, Collaboration, and Quality, November 5-6, Bolger Center, Potomac, Maryland The URL for this article is: http://www.wqusability.com/articles/consumer-health-usability.html |
 In my work at the
In my work at the  People can do already things with their bank, another high-security domain, that are amazing. It's amazing that I can go online and send wire transfers to any country in the world and don't even have to go into my branch. In fact, it's easier to do it online, because international wire transfers are usual in my rural branch.
People can do already things with their bank, another high-security domain, that are amazing. It's amazing that I can go online and send wire transfers to any country in the world and don't even have to go into my branch. In fact, it's easier to do it online, because international wire transfers are usual in my rural branch.  We can also easily forget that people in different roles may have very different
We can also easily forget that people in different roles may have very different 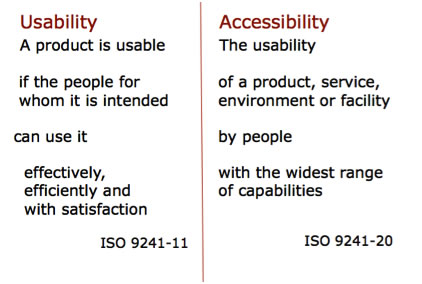 There’s a widely-cited ISO standard for usability (
There’s a widely-cited ISO standard for usability (